
In a groundbreaking development in the world of medical diagnostics, researchers at the University of Nottingham have unveiled a revolutionary test named ROBIN (Real-time On-site Brain tumour Investigation using Nanopore sequencing).
This test is capable of diagnosing brain tumours in under two hours. This is a dramatic improvement over the traditional diagnostic timeline of six to eight weeks.
While ROBIN was officially announced in May this year, its development spans several years of rigorous research and collaboration. The test has garnered significant media attention following its public unveiling. On 21 May, The Guardian reported on the breakthrough, highlighting the test’s potential to transform patient care by drastically reducing the time between initial presentation and diagnosis. The same day, The Scottish Sun echoed these sentiments, calling the test a ‘lifesaver’ and emphasising its high diagnostic accuracy. The Times also featured the story prominently, recognising the innovation as a major advancement in UK healthcare.
The ROBIN test leverages cutting-edge nanopore DNA sequencing technology to analyse tumour DNA extracted from biopsy samples. Once a sample is obtained during surgery, it is processed and analysed on-site, providing real-time molecular profiling of the tumour.

The sequencing data is then interpreted using a combination of machine learning algorithms and genomic databases to deliver a diagnostic result within approximately 90 to 120 minutes.
ROBIN has already showcased remarkable capabilities in clinical trials, achieving a 90% concordance rate with conventional diagnostic methods, indicating it can rival the accuracy of traditional lab-based pathology.
Adding to its innovation, the technology relies on compact nanopore sequencing devices which are small enough to fit in the palm of a hand, yet powerful enough to decode the entire human genome, underscoring both its portability and diagnostic strength.
The History Of Brain Tumour Diagnosis
Historically, diagnosing brain tumours has been a laborious and time-intensive process. Prior to molecular diagnostics, histopathological examination of tumour biopsies under a microscope was the gold standard.
1920s-1950s:
Between the 1920s and 1950s, diagnosing brain tumours was an arduous and often imprecise process. Physicians relied primarily on early imaging methods such as X-rays, which offered only limited anatomical detail, and basic microscopy techniques using stained tissue samples.
These diagnostic tools could reveal abnormalities in brain structure or cell appearance, but lacked the ability to distinguish between tumour types or provide deeper molecular insights. The interpretation of these images and samples was largely subjective, dependent on the expertise of the clinician, and often required invasive surgical biopsies for any degree of certainty.
The process was also time-consuming, with a diagnosis typically taking several days to weeks. Tissue samples had to be processed, stained, and examined under a microscope. These were procedures which involved considerable manual effort and were prone to variability.
Without access to modern molecular or genetic tools, treatment planning was based on general assumptions rather than precise tumour characterisation. As a result, patients often faced delays in receiving appropriate care, and the effectiveness of treatment was limited by the diagnostic tools of the time.
Despite these challenges, this period laid the foundation for advancements in neuropathology and imaging that would transform brain tumour diagnostics in the decades to follow.
1970s:
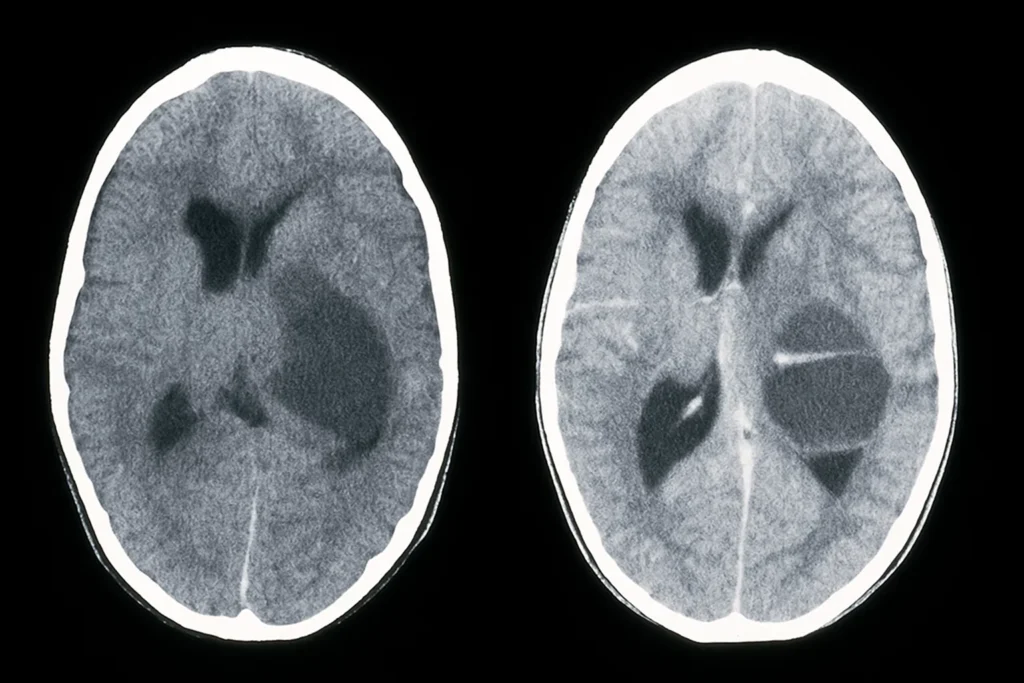
The 1970s marked a pivotal turning point in the diagnosis of brain tumours with the introduction of computed tomography (CT) scans. This technology revolutionised brain imaging by allowing clinicians to view cross-sectional images of the brain with far greater clarity and detail than ever before. For the first time, it became possible to localise tumours with precision, assess their size and position, and detect associated complications, such as swelling or bleeding.
CT scans dramatically improved diagnostic accuracy and reduced the reliance on exploratory surgery, which had previously been a common, yet risky, method for investigating suspected brain lesions.
This advancement significantly shortened the time required to reach a diagnosis and enabled more informed treatment planning.
CT scanning also laid the groundwork for the development of even more advanced imaging modalities, such as magnetic resonance imaging (MRI) in the following decade. In the context of brain tumour diagnostics, the 1970s represented the beginning of a new era; one in which imaging became central to understanding the structure and pathology of brain disease with unprecedented clarity.
1980s-1990s:
During the 1980s and 1990s, the advent and rapid advancement of magnetic resonance imaging (MRI) brought another major leap forward in the diagnosis of brain tumours. Unlike CT scans, which used ionising radiation, MRI used magnetic fields and radio waves to generate highly-detailed images of the brain.
This allowed clinicians to differentiate between various types of brain tissue and better distinguish tumours from surrounding healthy areas. As a result, MRI became an essential diagnostic tool. It is particularly valuable for identifying small or subtle lesions that CT scans might miss.
This era also saw the development of specialised MRI techniques, such as contrast-enhanced imaging and functional MRI (fMRI), which further refined diagnostic capabilities. These innovations enabled doctors to assess the tumour’s vascularity, potential malignancy, and proximity to critical brain structures. This information is vital for surgical planning and treatment decisions.
MRI’s non-invasive nature and improved resolution significantly reduced diagnostic uncertainty and improved outcomes for patients with brain tumours. By the late 1990s, MRI had firmly established itself as the gold standard for brain imaging, reshaping the diagnostic landscape in neurology and oncology.
2000s:
In the 2000s, the field of brain tumour diagnosis underwent a major transformation with the rise of molecular pathology. This new approach moved beyond the traditional reliance on histology and imaging, incorporating advanced techniques, such as immunohistochemistry and genetic testing. The inclusion of these techniques allowed for a more detailed and accurate understanding of tumour biology to be given.
By analysing the expression of specific proteins and identifying genetic mutations or chromosomal alterations, clinicians were able to classify brain tumours into more precise sub-types. This molecular-level insight enabled more accurate diagnoses, allowed for better prediction of tumour behaviour, and offered clues about how a tumour might respond to specific treatments.
The integration of molecular data revolutionised treatment planning, giving rise to the era of personalised medicine.
Molecular pathology also laid the groundwork for the development of new treatment protocols tailored to individual tumour profiles, significantly improving patient care. By combining traditional pathology with molecular diagnostics, the 2000s marked a critical shift toward a more biologically-informed approach to diagnosing and managing brain tumours.
2016:
In 2016, the World Health Organisation (WHO) introduced a landmark update to its classification of central nervous system (CNS) tumours, marking a pivotal shift in the way brain tumours were diagnosed and understood.
For the first time, molecular markers were incorporated alongside traditional histological features in the official diagnostic criteria. This meant that tumours were no longer defined solely by how they appeared under the microscope, but also by their genetic and molecular profiles, ushering in a new era of integrated diagnosis.

he revised classification recognised that tumours with similar microscopic features could behave very differently depending on their molecular characteristics, and vice versa.
However, despite these advancements, traditional methods still involve sending tissue samples to specialised labs, with results taking weeks. This delay can impact treatment planning and outcomes, especially in aggressive cancers like glioblastomas.
What This Means For The Future
ROBIN promises to streamline this process, allowing for immediate decisions to be made. Surgeons can determine tumour type and grade while the patient is still in the operating theatre, potentially reducing the need for repeat surgeries and expediting the initiation of targeted therapies.
With plans for NHS implementation within the next year, ROBIN could soon become a standard part of neuro-oncological care in the UK, setting a new benchmark for diagnostic speed and accuracy.
As the technology matures and scales, its potential application may extend to other cancers and critical conditions, heralding a new era of ultra-rapid, real-time diagnostics in global healthcare.